In this article, we theorize the impact of risk logics on professional work and workers, developing an analytical framework, which we illuminate with examples from health and social care. The development of such analyses of experiences and practices is important given the proliferation of risk logics within organisations where many profession(al)s work.
Studies in the sociology of professions have long emphasised the centrality of uncertainty to the emergence and maintenance of professional and occupational groups, and particularly the constraints and benefits of uncertainty, or “indeterminacy,” for gaining cultural authority and exclusive access to labour markets (Fox, 1980; Freidson, 1974; Jamous & Peloille, 1970; Nilson, 1979). These broader power dynamics shape how individual professionals go about their work. Parsons (1951) drew attention to the role of emotion-based practices as a means of handling uncertainty (at the micro-level) which, in turn, lead to orientations towards uncertain futures which are implicitly “magical” and enhance the functioning, authority and power of professions (Good et al. 1990; Fox, 2000, p. 410). Fox extended these Parsonian interests in her work assessing the “social, cultural, emotional, and moral and spiritual meaning[s]” of uncertainty for professionals (Fox, 2000, p. 410), as these both shape and emerge out of micro-level practices, experiences, and interactions.
Recent studies in the sociology of risk and uncertainty, meanwhile, have specified different ways of handling uncertainty, and their related meanings: Zinn (2008) and Alaszewski (2015) contrast hope and magic-oriented approaches to managing uncertainty with the more rational-calculative (often probabilistic) approach of risk, noting that most experts combine both rational and non-rational bases of going forward amid uncertainty, as well as “in-between” strategies such as trust, emotions, and intuition (Zinn, 2008). While trust and hope are prominent within classic accounts of professional power and work (Parsons, 1951), it is risk which is increasingly (re)defining the logics of the organisations within which many professions now work (Power, 2004; Rothstein, 2006).
Where evidence-based practice is characteristic of a shift in what it means for professionals to know and act (Fox, 2000), then risk management represents the archetype of this refashioning of decision-making—drawing upon the pooling of population-level data on factors, peoples, and outcomes in terms of probabilities and related causal understandings. Shaping and governing professional work in line with risk logics involves reconfiguring hierarchy and accountability (Noordegraaf, 2011), where Fordist standardisations of professional work (Harrison, 2002), reconfigurations of blame (Douglas, 1992; Warner, 2006) and a related intensification of (self-)surveillance (Deetz, 1997; Fournier, 1999) have become common responses to risk. These trends are also related to “contemporary pressures towards greater coherence, transparency and accountability” (Rothstein, 2006, p. 215), following politicisation of professional fallibility (Alaszewski, 2002; Power, 2004).
Once it has been introduced within commercial or new public management settings, risk has a tendency to proliferate (Power, 2004). Risk governance is attractive through its ostensible efficiency (Garland, 1997), its redistributing of blame and rationalising of failures as a defensive form of governance (Rothstein, 2006), and its ostensibly technical nature which belies political machinations (O’Malley, 1992). All of these assist the successful managing of reputational risks faced by organisations (Rothstein, 2006). Yet the development of risk management gives rise to further risks, whereby an “increasing emphasis on scrutiny and accountability has amplified and routinized the management of institutional risks, as failures have to be recorded, potential failures have to be anticipated and new categories of failure are defined. From this perspective, ‘good governance’ gives rise to risk itself” (Rothstein, 2006, p. 217).
In this context, risk is an increasingly common and central basis of both decision-making and communicating within many kinds of professional practice, and in the evaluation of professionals’ work (i.e., the extent to which they minimize risk). For instance, there has been a shift in accountants’ and auditors’ practices towards the identification, assessment, and detailed reporting of risks (Power, 2000, p. 117), the reshaping of policing and logics of stop-and-search through statistical crime mapping and other factor-based strategies (Chainey & Ratcliffe, 2013, p. 174; van Eijk, 2017), the assessment of potentially dangerous patients by psychiatrists in terms of risk factors (Castel, 1991; Szmukler, 2003), and the use of face-to-face communication interventions of public health professionals targeting “at risk” groups and individuals (Bunton, Burrows, & Nettleton, 2003).
Given the reconfiguring of professional power and work within various private and public organisations (Noordegraaf, 2011), the proliferation of risk within these organisations recasts professionals’ handling of uncertainty. This has implications for the nature and experience of work, which, as noted above in relation to Fox and Parsons, is important in that a) practices and experiences of professional work are important objects of study in and of themselves; and b) practices and experiences in relation to uncertainty both reflect and feed back into the broader dynamics of professional authority and organisational governance.
The aim of this article is to outline a theoretical framework for analysing risk work. By “risk work" we refer to the practices of professionals (and those assisting professional work) dealing directly with clients, where the management of risk—through assessing, intervening, advising and/or communicating—has become a key and (in some cases) (re)defining logic of everyday work. Our approach to risk work is especially focused upon the material and embodied practices which enable this work to “get done” (see Horlick-Jones, 2005), and what this means to lived experiences of work and (para)professionals’ identities (cf. Power, 2016).
First, we explore how—amid a range of research on risk across sociologies of professions, work, risk, and health and social care—these latter concerns with pragmatic practices and negotiated identities remain relatively neglected. We then introduce a model of three key features of risk work and the tensions which emerge as they are combined in practice (see Figure 1), alongside an understanding of processes by which these tensions may become more explicit or remain latent within everyday working experiences and practices. Our arguments are grounded in an extensive review of related literatures (Gale, Thomas, Thwaites, Greenfield, & Brown, 2016), our own recent empirical studies (see, for example, chapter 5 of Brown & Calnan, 2012; Gale, Dowswell, Greenfield, & Marshall, 2017; Gale, Kenyon, MacArthur, Jolly, & Hope, 2018, Veltkamp & Brown, 2017) and pilot work to test our emerging theory, and are presented alongside a reworking of key features of post-phenomenological social theory. The final section points to some further possibilities for extending this model and lines of research in relation to two fundamental questions: first, how is risk work practically and pragmatically accomplished amid the residual uncertainties, which emerge when handling risk? And second, what is the lived experience of client-facing (para)professionals as they handle risk as part of their everyday practices? The model and research possibilities are salient to a range of professions and professional work that operate within a risk society but, by way of exposition, we focus below on professionals oriented towards health and social care.
Existing research on the wider context of risk and organisations
Within health and social care contexts, risk is frequently invoked by practitioners and researchers as they seek to better understand and intervene in probabilistic relationships between an array of ostensible “causal” factors and manifestations of morbidity, mortality or harm (outcomes in other professional domains would include criminal activity, financial losses, young people’s radicalisation, and so on). Moreover policy-makers and managers are increasingly prone to couching the logic and legitimacy of their (re)organising of various healthcare contexts in terms of the management and reduction of risks (Rothstein, 2006). Sociologists of health and medicine have responded to these tendencies with an expansive body of research which critically considers and illuminates the development of risk knowledge and its application within healthcare organisations. These studies, as with sociological studies of risk and uncertainty more generally, have tended to focus on the production of risk knowledge (Jasanoff, 2004; Møller & Harrits, 2013), its expansion and implementation across healthcare and wider public sector organisations through governance systems (Flynn, 2002; Power, 2004, 2016; Rothstein, 2006), the ways in which risk is understood and communicated (Engdahl & Lidskog, 2014; Scamel, 2011), and (perhaps above all) the various ways in which risk “makes” or recasts the patient subject (Castel, 1991; Novas & Rose, 2000; Peterson, 1997).
The experiences of client-facing practitioners—who, with varying degrees of autonomy, apply risk knowledge and risk-framed policies, within and between health and social care organisations (Lipsky, 1980; Gale et al., 2017), and in interactions and relations with these patient subjects—have remained rather neglected however. Few studies have peered into the messy world of how such risk work actually “gets done” (Harrits, 2016; Horlick-Jones, 2005) and still fewer have considered the lived, embodied experiences of what it means to accomplish everyday risk work (Gale et al. (2016) and Harrits and Møller (2014) analyse decision-making and identity among front-line prevention workers but not in relation to risk).
In sociological approaches to work, concepts of risk and uncertainty have been applied to describe the location and experiences of employees within the wider labour market, and how those might be stratified (Beck, 2009), rather than how workers embody and deploy risk knowledge itself, or their experiences of doing so. Literature on the professions has similarly paid little attention to the recasting of occupational or professional identities and values (Evetts, 2009; Nancarrow & Borthwick, 2005) produced by the growing dominance of risk logics in organisations across many sectors.
Where workers have been the focus, attention has been placed on practices of working within risk governance frameworks, especially in terms of accountability pressures and so forth (Warner & Gabe, 2004). This research has tended to focus on the formats and logics of such governance and accountability frameworks or upon workers’ experiences of reporting on and accounting for their work, rather than the practicalities, experiences and (potential) tensions in the handling of uncertainty via risk within everyday work practices (for exceptions, see Fischer & McGivern, 2016; Horlick-Jones, 2005; Nading, 2013; Warner, 2006; two chapters within Power, 2016 though the book overall focuses on organizational contexts away from the frontline).
A small literature, alongside our own research, has, however, enabled us to identify various practices which we see as distinctive to risk work in health and social care contexts. These studies consider how risk gets translated into different contexts (see Arribas-Ayllon & Sarangi, 2014; Burton-Jeangros, Cavalli, Gouilhers, & Hammer, 2013), how practitioners intervene to minimise risks in practice (see Cabral, Lucas, Ingram, Hay, & Horwood, 2015; Cricco-Lizza, 2010), and/or how caring is carried out amid (or in spite of) contexts characterised in terms of risk (see Broom, Broom, & Kirby, 2014; Iversen, Broström, & Ulander, 2017). These three features of risk work—interpreting risk knowledge, intervening to minimize risk, and handling social relations and interactions—are illuminated in these studies alongside some connections between them (Gale et al., 2016). In the following section we go further to conceptualise these three features before arguing that we must consider the interconnectedness of these features of risk work in a systematic manner and, moreover, to address how they often stand in tension with one another.
Core features of risk work
In its narrowest sense, risk can be defined as “the probability that a particular adverse event occurs during a stated period of time, or results from a particular challenge” (Royal Society, 1992, p. 2) and is applied straightforwardly to calculate the likelihood of health, illness or intervention outcomes. Yet there remains a range of factors, which render this risk knowledge less than straightforward and, indeed, rife with tensions. These factors can help us to understand the intractability of enduring uncertainties and the subsequent limits of expertise. Interrogating this Royal Society definition, Heyman, Alaszewski, and Brown (2013, p. 1) deconstruct risk to acknowledge: the range of values present when deciding what is “adverse”; the categorising which is always implicit when grouping ostensibly similar “events” together and linking these to homogenised groups of risk factors (people, places, and so forth); the time frames employed which (contrary to the definition) are rarely explicitly “stated”; not to mention various ways in which statistical probabilities are invoked. So, while evidenced-based medicine and epidemiological studies have amassed a vast array of understandings of probabilistic relations between factors and outcomes, these four fault-lines—values, categories, time frames and interpreted probabilities (Heyman et al., 2013)—inherent to risk are always lurking beneath the surface and may emerge uncomfortably within specific settings.
In thinking analytically about how the management of uncertainty through risk may lead to further ambiguity, it is useful to return to various research studies on how professionals deal with uncertainty (as introduced above). The strength of these approaches has been their ability to connect phenomenological accounts with organisational analyses (Brint, 1993); their acknowledgement of the extent of discretionary (“street-level,” Lipsky, 1980) decision making (Fox, 1980; Nilson, 1979); and their sensitivity to the manner by which experiences of, and rewards for, the instrumental handling of uncertainty vary greatly depending on a worker’s position within the broader occupational hierarchy (Nilson, 1979).
Renée Fox has developed a significant body of work which explores in detail how practitioners learn to handle uncertainty, for example with regard to the limits of scientific knowledge more broadly, the limits of the individual worker’s understanding, as well as the ambiguity in distinguishing between the two (Fox, 1980, p. 5). More recently, Fox has argued that changes in medicine over recent decades have reconfigured the uncertainties and risks that professionals and the public face. Perhaps most saliently to the present concern with risk work, Fox explores the growing commitment to evidence-based medicine (EBM). She argues that it produces “epistemological uncertainty,” that is to say, uncertainty about the “nature of good clinical research, good clinical practice and the relationship between them” (Fox, 2002, p. 245). At a clinical level, evidence-based medicine seems to provide clinicians with a level of certainty—with the notion of “best evidence” available—from which to act. However, Armstrong (2007) has argued that, while EBM claims to have reduced indeterminacy, it is better understood as merely shifting the “problem”of uncertainty to a wider policy arena that involves interpreting evidence. Fox (1980, p.1) explains that medical progress has also “helped to reveal how ignorant, bewildered, and mistaken we still are in many ways about health and illness, life and death.” This paradox is echoed in later sociological narratives of a late-modernity (Giddens, 1990; Beck, 2009), where an increased propensity for experts and others to handle the uncertain through probabilistic inferences has emerged alongside an intensification of doubt in expertise and elites (Jasanoff & Simmet, 2017). We now move to trace the sources of these underlying tensions in risk knowledge back to three underlying features of risk work (see Figure 1).
Figure 1.
Core concepts and tensions in risk work
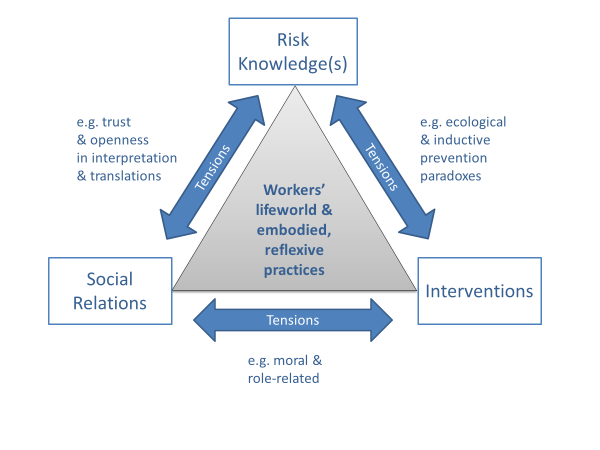
Risk knowledge(s)
In order to build or amass risk knowledge in the first place, researchers must pool together large numbers of cases and outcomes. This involves the “disembedding” of these observations from space and time (Giddens, 1990) and has become integral to the creation of new scientific knowledge. However, it creates a wholly different form of medical knowledge (Carter, 1995) from the in-depth case studies and experiences which remain to a large extent a common basis of medical decision-making and knowing (Eraut, 2000; Lave & Wenger, 1991).
This different type of technology or knowledge, through which medical practice is increasingly framed, leads to new forms of social relations for those applying it (Beck, 2009; Will, 2005). Castel (1991) exposes some of the formats of these new relations in the context of mental health social work and psychiatry, where the patient is known and assessed differently—as a collection of abstract risk factors—thus shifting the locus of understanding away from the individual person. Moreover the nature of organisation and intervention is also reconfigured by this new technology of risk:
The presence of some, or of a certain number, of these factors of risk sets off an automatic alert. That is to say, a specialist, a social worker for example, will be sent to visit the family to confirm or disconfirm the real presence of a danger, on the basis of the probabilistic and abstract existence of risks. One does not start from a conflictual situation observable in experience, rather one deduces it from a general definition of the dangers one wishes to prevent. (Castel, 1991, pp. 287-288)
This is just one of several ways in which new forms of risk knowledge may lead to changing dynamics within the interactions and relationships between professionals and patients. Nevertheless, other non-probabilistic forms of knowledge continue to inform practitioners’ understandings of risk and negotiation of uncertainty – such as tacit, embodied and intuitive forms of knowledge and these different ways of knowing can sit alongside or in tension with each other (see MacLeod & Stadnyk, 2015).
Interventions
The generation of new forms of risk knowledge may also lead to wholly new interventions and relations, whereby new “at risk” publics become the focus of public health interventions (Armstrong, 2012), following the publication of research studies or policy guidance categorising them both as a meaningful “group”—due to their locality, age, gender, ethnicity, culture, educational level, health status, or other characteristics—and “at-risk.” Not only may these interventions require different logics of action, in terms of knowledge and decision-making, but these interventions may extend professionals remit into new domains—for example where health professionals are required to assess risk of radicalisation (Chivers, 2018)—or where paraprofessional or lay workers are brought in to deliver interventions based on emerging understandings of what works, what can be afforded, or a combination of the two (Hartley, 2002; Singh & Chokshi, 2013).
We use intervention here in a broad sense as, while this may involve concrete actions such as undertaking emergency pre-emptive surgery or sectioning a service-user amid a psychotic episode, intervening may alternatively involve communicating, advising and educating about (probabilistic) links between behaviours and outcomes, or a (para)professional may merely be assessing risk (collecting and interpreting information) as the potential basis of future intervention (for example, as a health visitor or paediatrician meeting a vulnerable family, Veltkamp & Brown, 2017).
Intervening in these different ways usually involves the reworking or translation of abstracted risk knowledge and/or related guidelines back into a concrete social context; which can have unintended consequences (Heyman et al., 2013) and even devastating effects (for example, in child-safeguarding—Munro, 2010). It is at such moments of embodied interaction, amid material settings and relations, that the categories (for example, understandings of “at risk” groups), values (for example, notions of what is a good outcome) and moralities (what is considered responsible action) which are intrinsic but often implicit within abstract risk knowledge may become explicit and awkward (Cricco-Lizza, 2010; Mishra & Graham, 2012).
Social relations
The challenges of knowledge interpretation in the context of specific interventions may also create conflicts of role and tensions in practitioner-service user relationships (Fox 2002; Currie, Finn, & Martin, 2010). Intervening on the basis of risk knowledge—whether it be through communicating the risks associated with continuing particular “lifestyle” practices, acting to remove a child from a family, or organising the hospitalisation of a person experiencing severe mental health problems—is always a moral act (Douglas, 1992), with often profound consequences for the interaction at that moment as well as for the relationship with that person, group and/or patient in the longer-term. These consequences will play out in opening up or limiting the possibilities for working and interacting with these individuals or groups in the future, particularly regarding the quality of communication which will be possible. Child health care professionals, for example, are aware that their intervention (communicating/advising) at a particular moment may have implications for whether a family remains “in view” or breaks off contact from the service (Veltkamp & Brown, 2017). The style and content of communication will, therefore, have important consequences for practitioners’ ability to grasp the complex dynamics of risk factors facing a particular family in the future.
Paradox and fallacy in risk work
The tensions we have explored when intervening to minimise risk based on current risk knowledge—which in turn impacts on the nature of professional relationships with clients and (full circle) on the understanding and knowledge of risk—helps make apparent how the values and morality bound up with risk framing and categories are deeply interwoven within probabilistic knowledge and inference. Heyman’s “inductive prevention paradox,” whereby the practice of intervening to reduce risk gradually comes to warp or undermine the quality of knowledge (either probabilistic or tacit) on which interpretations are made (see Heyman et al., 2013), neatly captures the tensions in knowledge brought about by intervening.
Meanwhile, the problems of intervening brought about by knowing through a lens of risk are partly captured within an “ecological fallacy” of risk (Heyman et al., 2013), whereby risk knowledge about probabilistic tendencies across populations is much less useful in predicting outcomes for any specific individual. This means that while, from a population-level perspective, there is a case for prescribing statins (to reduce levels of coronary heart disease), GPs’ considerations of the relative individual benefit (and costs) for the person in front of them renders decision-making less clear cut (Will, 2005). Intervening (prescribing) or not, and how this is then explained amid interactions with the patient, raises a range of practical and moral questions. This is apparent where GPs acknowledge that they would not be prescribed statins themselves, preferring to make lifestyle changes (Gale, Greenfield, Gill, Gutridge, & Marshall, 2011), or where patients resist the discourses of “patient choice” and “risk” because they are unwilling to be cast as “pill-takers,” unless they can construct an “idea one can live with” about “needing” medication now (Polak, 2016).
These two more specific problems are a useful means of starting to “unpack” the more general paradox noted by Fox (1980, noted earlier) whereby the refining of technologies for handling uncertainty results in an ever more intense experience of awkward residual uncertainty (see also Beck, 2009, p. 18; van Asselt & Renn, 2011). These and other paradoxes—as with the wider tensions sketched in this section—may emerge within, and trouble, the decision-making practices and experiences of professionals in various ways.
In this section we have sketched three core features of risk work—risk knowledge(s), interventions and social relations—their connectedness, and some potential tensions (the tensions referred to here are not intended as an exhaustive list) existing between them. In particular, we assert that the new technologies of risk have important consequences for the social and moral relations involved in health and social care work. In the midst of these knowledges, practices, relations and tensions are the workers themselves—their lived experiences, lifeworlds, and identities (see Figure 1). In this sense, following one of the basic schemes of risk theory (see Beck, 2009), we can consider that new technologies lead to new social relations which in turn lead to new experiences of self. While processes around the patient- or public-self have been considered in quite some detail, the experiences and identities of those handling risk in their work have remained largely and, we argue, problematically neglected.
Uncovering and (partially) resolving tensions within risk work
Having sketched the three basic features of risk work and introduced the phenomenon of tensions inherent to these practices, we now move to consider more closely the nature of these tensions. We are interested in both how the experiences of tensions relate to (changes in) the practices of how risk work is accomplished, and how these tensions may remain partially veiled; never being fully exposed or confronted and thus remaining awkward in experiences of everyday work (see, for example, Thomas, 2016). Or indeed there are other instances where one might expect a controversial or apparently incongruous risk management policy—such as requiring health professionals to screen for risk of radicalisation—to create all kinds of tensions for professionals, but where this policy can be experienced relatively unproblematically through its incorporation into familiar professional discourses (Chivers, 2018).
Recent work in medical sociology, the sociology of risk and uncertainty and related disciplines such as anthropology have produced quite some evidence that workers within client-facing occupations in health and social care continue to face an array of tensions in their everyday work (see Nading, 2013, Warner & Gabe, 2004), even if this is often not the central focus of the research.
In handling risk knowledge within contexts of childbirth, for example, Scamell (2011) refers to the tensions experienced by midwives who she describes as treading a difficult line between facilitating a “normal” process of childbirth while simultaneously handling a situation saturated in “latent risk.” In another study, Scamell and Stewart (2014, p. 97) explore tensions involving probabilities and the difficulties inherent in interpreting “low-probability but high consequence” risks within specific birthing situations. In these two studies, the intervention and interactional aspects of this risk work, where an appearance of normalcy and calm are understood as vital for interactions with labouring women, is described as involving tensions around the categorisation of situations (in terms of “risky” or “normal”), the organisational and professional valuing of risk-aversion and normal birth, and the handling of the various time-frames imposed via a safe birthing schedule.
While there are of course aspects of midwifery work which are highly specific to this profession, we argue that quite diverse forms of risk work may share an array of similar conundrums, which we can consider in terms of our three key features of risk work, the tensions which emerge around these, and the questioning of the key features (see Figure 2). More specifically the three features of risk work can be considered as configuring professionals’ lifeworlds, involving processes of meaning-making and knowledge construction (culture), professionals location amid social relations (society) and selfhood (identity) (Habermas, 1987). These three layers of workers’ lifeworlds may, respectively, involve the questioning of risk work in terms of
-
the truth of risk knowledge—in light of shared cultural understandings of risk workers’ meaning frameworks;
-
the legitimacy of interventions—as configured by risk workers’ membership of multiple social networks (professional teams, for example) and their position within these;
-
the authenticity of experiences within relations and interactional practices—in light of the socialised individual identity of workers themselves (see Habermas, 1987, pp. 138148; Brown, 2016).
Figure 2.
Tensions amid risk work may lead to workers questioning key features
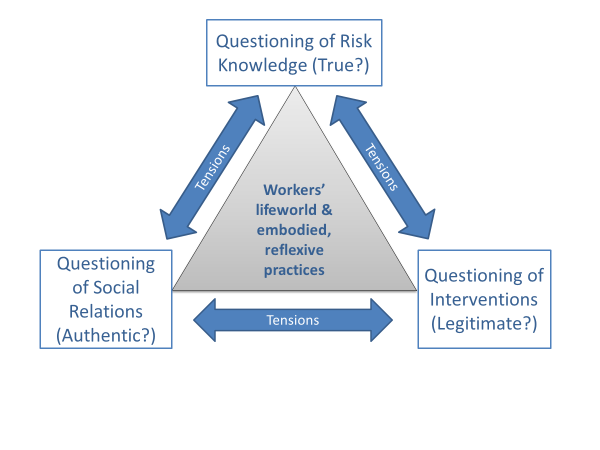
The interwoven nature of the three core features of risk work can mean that tensions around legitimacy of intervening (for example) may spark further questioning and tensions regarding truth and authenticity. Yet alternatively these interwoven features may also form the basis of the (more or less temporary) rationalisation, resolving or “bracketing off” (Brown, 2016; Chivers, 2018; Habermas, 1987) these tensions—where tensions involving the authenticity of social relations, for example, are accepted due to more positive considerations of truth and legitimacy. This framework helps us to organise, understand and connect an array of processes by which the various fault lines inherent to risk (noted above) may be uncovered and (partially) re-covered amid everyday practices; within and outside of the work place.
In various forms of screening, for example, conflict and doubt may emerge over the evidence, ontological foci and thus truths behind risk work at the population level (Timmermans & Buchbinder, 2012; Solbjør, Skolbekken, Saetnan, Hagen, & Forsmo, 2012). Despite these conflicts, the interventions may still be experienced as highly authentic due to individual level success stories (detection of cancer, for example), alongside a worker’s identity and history of training as a public health specialist, and the enduring legitimacy of the value of intervention among professionals.
There may be other contexts, meanwhile, where guidelines ring true in terms of evidence of reducing mortality or morbidity at the population level but which seem less legitimate and authentic when invoked within individual cases and interactions. Examples here include children who have experienced vaccine damage or adults who experience side-effects when using statins designed to reduce their “cardiovasular risk” when they previously felt “well.” How these types of individual-level tensions are experienced and negotiated by practitioners has not, to our knowledge, been considered in the literature. However, relevant empirical findings include those healthcare practitioners who do not follow the same advice they give patients (Gale et al., 2011; Raude, Fischler, Lukasiewicz, Setbon, & Flahault, 2004), or who do follow it but with ambivalent feelings (Armstrong-Hough, 2015, Thomas 2016).
Such problems of legitimacy and authenticity may be voiced and challenged among colleagues and management, or alternatively may be avoided through the informal reinterpretation and reconfiguring of risk in ways which help maintain or protect its apparent truth basis, legitimacy and/or authenticity. As Timmermans and Buchbinder (2012, p. 210) found in their research on screening for genetic birth “disorders,” even when doubts are cast about the value (cost-benefit) of screening, “it is difficult to turn back the screening momentum precisely because the [hands-on] work in the clinic buffers ontological incompatibilities.” There is, therefore, also much to gain from looking beyond lifeworld dynamics towards questions of everyday embodied and reflexive practices among professionals, where the reproductive tendencies of the (professional) habitus (Bourdieu, 1977, Broom et al. 2014) may be an alternative or complementary means of explaining the “momentum” behind the unquestioned continuation of interventions and practices—regardless of tensions of truth, legitimacy and authenticity—and the relative lack of tensions amid seemingly contrary practices (see Chivers, 2018).
Two overarching questions emerge from our framework that may serve to orientate future research. They relate to embodied professional practices, and especially how the tensions inherent in risk work are handled while still getting the job done: first, how is risk work materially and practically accomplished amid the residual uncertainties which emerge when handling risk? And second, what is the lived experience of client-facing (para)professionals as they handle risk as part of their everyday practices?
Analysing risk work and its tensions
In this third and final part of our argument within the scope of this article, we sketch a range of analytical trajectories which develop out of our theorisation of risk work introduced above. The most obvious line of investigation is into the various processes by which tensions emerge, remain (partially) hidden or are reconciled. Despite the tensions and anomalies which begin to surface amid risk work, the habits and learned practices of workers, and various lifeworld processes may prevent these tensions from being fully exposed and subjected to rational scrutiny. Those carrying out risk work continue, more or less informally, to pragmatically muddle through and adjust their practices in relation to risk knowledge, the interventions they are part of and their social relations with clients, but with these tensions continuing to bear on their everyday experiences (Thomas, 2016).
These pragmatic practices may involve awkward experiences of tensions—daily or occasionally—however it may be the case that processes occurring amid and in relation to the lifeworlds of these professionals resolve or veil these tensions. We saw in the previous section how (in)authenticity, (il)legitimacy and the affirming or problematisation of “truth” about risk can feed back into one another, either amplifying or defusing tensions. These lifeworld dynamics of risk work will be shaped by public sphere debates, interactions with colleagues and clients, and/or individual reflection where tensions may be pragmatically and more or less deliberatively “bracketed off” (Brown, 2016). Embedded within wider institutional norms and pressures, these dynamics may be oriented towards further and deepening understanding, and/or more “strategically” to meeting targets and getting the job done (Habermas, 1987). An exhaustive list of possible empirical manifestations of these dynamics is not possible here. Instead, we use three brief concept-based examples to show how tensions remain veiled as mere tensions, instead of resulting in more explicit contestations:
x) Practitioners’ deference to expert knowledge: Although experiences within and outside work contexts may lead to a questioning of the truth of risk knowledge, frontline practitioners may assume or argue that scientists, their managers and/or more senior clinicians “know what they are talking about” (see Fairhurst & Huby, 1998). In this way power/knowledge as hierarchy, and the practical logic (Bourdieu, 1977) of deferring to higher status professionals leads to a more or less resigned acceptance (despite niggling questions), with tensions being either explained away or remaining unvoiced and so the truth of risk knowledge remains relatively uncontested at the local level. Of course, the relative hierarchy or flatness of the organisation and a practitioner’s position within this, alongside aspects of the worker’s identity and presentation of self, will also bear upon the level of deference or open questioning.
y) Practical obligation amid organisational logics: Questions may well exist about the truth of knowledge and/or the legitimacy of interpretations of risk but pressures of time—amid an underlying organisational logic embedded within economic imperatives—may make a more thorough critical reflection and questioning impossible. Practitioners have case-loads to get through or workshops to deliver. They may feel that they are not paid to question but to deliver (Thomas, 2016). Where risk knowledge is experienced as problematic in terms of truth and/or legitimacy then, rather than being challenged, other informal ways of handling uncertainty are drawn upon—such as alternative heuristics and/or trust (Zinn, 2008). These types of approaches mean that the knowledge-related tensions remain unresolved, as well as leading to further potential tensions between formal compliance and informal logics (Brown, 2011; Horlick-Jones, 2005).
z) Patients’ and publics’ deference to the expertise and role of practitioners: The client-facing nature of risk work requires us go beyond analyses of working practices themselves and to consider the interactive and communicative dynamics, which also play an important part in keeping tensions concealed. Kihlström & Israel (2002, p. 212; see also Scambler & Britten, 2001) explore various ways by which welfare state professionals may handle interactions—either deliberately or unwittingly—in ways which can either enhance open exchange and mutual understanding (communicative action), or which inhibit openness due to a professional’s focus on getting things finished or getting their way (strategic action). Unwitting strategic action and/or implicit forms of power (deference to experts, for example) may lead to professionals experiencing interactions as authentic and legitimate when the experience of the client is very different. While trust may in some cases enhance open frank communication, when trust is more instrumental and deferential (Brown & Calnan, 2012), patients may assume that professionals are acting in their interests and/or feel obliged not to question. Even when abstract others such as researchers or pharmaceutical companies are distrusted (Brown & Calnan, 2012), forms of trust in known experts, such as family doctors, may still impede the communication of doubts and questions while obliging awkward “cooperation” (Ward, Coffey, & Meyer, 2015).
Risk work can thus be further explored by engaging in more detailed considerations of lifeworld processes (than is possible in this article—see Brown, 2016; Chivers, 2018), alongside the interactions between lifeworlds and instrumental actions and structures oriented towards success (the “system”—see Chivers, 2018; Habermas, 1987; Scambler & Britten, 2001) and the practical logics and habitual actions that guide professional work (Brown, Crawford, Gilbert, Gilbert, & Gale, 2014; Bourdieu, 1977) and the response of clients to it. These conceptual frameworks may thus afford a useful set of analytical and conceptual tools, though critical handling of these frameworks is also necessary, for example to emphasise the importance of interactions (Brown 2011) or the multiple identities which bear upon work (Chivers, 2018; cf. Habermas, 1987).
Conclusion
We began this article by suggesting that, amid a wider sociological literature around professions and work, and risk and uncertainty, the specific practices and experiences of those handling uncertainty through risk in their everyday work have remained neglected, despite the proliferation of risk management and related work forms across a wide range of organisations within which various (para) professionals are employed.
In developing a conceptualisation of this risk work, we have identified its three core features—risk knowledge, interventions, and social relations. It is the interaction between these three features, which is central to understanding the dynamics of practices and experiences of risk work, whereby important tensions may be generated. This may lead to various fault lines underpinning risk (values, categories, probabilities, timeframes) becoming uncovered; potentially with awkward consequences. We have explored how such tensions may or may not become explicit, partly as a result of pragmatic everyday working practices by which the difficulties of handling uncertainty through risk are “resolved” and normalised.
Tensions emerge between the key features of risk work, for example as risk knowledge is shaped into an intervention, or as workers seek to maintain (good) relationships when intervening (see Figure 1). These tensions may, in turn, result in workers questioning one or more features of risk work—risk knowledge (in terms of truth), interventions (in terms of their legitimacy), and/or social relations (in terms of authenticity) (Figure 2). Where the experience of tensions leads to questioning, then this is likely to have an impact on everyday practices in terms of how risk knowledge, interventions and social relations are handled. This will in turn (re)shape experiences. The relationship between practices and experiences is further complicated by the potential veiling of tensions through a range of processes related to professionals’ lifeworlds and embodied experiences of work. Veiled tensions also impact on everyday experiences of work.
Our theorisation of risk work is intended as a foundational framework for research into the embodied and reflexive practices of “client-facing” professionals and paraprofessionals charged with identifying, handling and minimizing risks in their everyday work. Professional practices are important in their own right, as features of professional work, but they also can teach us about professional power dynamics at organisational and societal levels. In this article, we have illustrated our theorization with examples from health and social care, although the range of professionals and others undertaking risk work in their everyday employment is, of course (and as noted in the introduction), much broader.