University of Lapland, Faculty of Education
Centre for Media Pedagogy (CMP)
Rovaniemi, Finland
Email: firstname.lastname@ulapland.fi
The aim of this study was to design a pedagogical model for a simulation-based learning environment (SBLE) in healthcare. Currently, simulation and virtual reality are a major focus in healthcare education. However, when and how these learning environments should be applied is not well-known. The present study tries to fill that gap. We pose the following research question: What kind of pedagogical model supports and facilitates students’ meaningful learning in SBLEs? The study used design-based research (DBR) and case study approaches. We report the results from our second case study and how the pedagogical model was developed based on the lessons learned. The study involved nine facilitators and 25 students. Data were collected and analysed using mixed methods. The main result of this study is the refined pedagogical model. The model is based on the socio-cultural theory of learning and characteristics of meaningful learning as well as previous pedagogical models. The model will provide a more holistic and meaningful approach to teaching and learning in SBLEs. However, the model requires evidence and further development.
Keywords: simulation-based learning environment, socio-cultural theory, meaningful learning, design-based research, case study, facilitators, students
Simulation-based learning has been proven to be effective, experiential and fun (Brewer, 2011; Cook et al., 2011; Konia & Yao, 2013). Simulation technologies enhance learning and affect clinical practice (Cook et al., 2011; Eaves & Flagg, 2001; Hayden, Smiley, Alexander, Kardong-Edgren, & Jeffries, 2014; Konia & Yao, 2013; Paige, Arora, Fernandez, & Seymour, 2015). However, when and how these learning environments should be applied is not well-known. As Ker (2012, p. 346) observed: “There is a need to ask more how and why questions as opposed to ‘does this work?’ or ‘which is better?’”
The purpose of this study was to understand teaching and learning in simulation-based learning environments (SBLEs) in healthcare in order to find answers to the how question. These advanced, complex and expensive environments will enhance learning only if they are used appropriately. The specific aim of this study was to design a theoretically and empirically justified pedagogical model for a SBLE in healthcare (Keskitalo, 2015). The purpose of the pedagogical model was to emphasise the learning theories that will eventually enhance students’ meaningful learning in these unique contexts. We created multiple research tasks in order to answer the following research question: What kind of pedagogical model supports and facilitates students’ meaningful learning in SBLEs? The study used the design-based research (DBR) (Brown, 1992; Collins, Joseph, & Bielaczyc, 2004; Design-based Research Collective, 2003) and case study approaches (Gray, 2004; Yin, 2013).
The first cycle, designing the pedagogical model (Keskitalo, Ruokamo, & Väisänen, 2010), was conducted at the simulation centre of Arcada University of Applied Sciences (Helsinki, Finland) from April to May 2009. During the case study, various methods were used to collect data from paramedic students and facilitators. The first cycle resulted in a redesigned pedagogical model, which was evaluated during the second cycle of the design-based research. In this paper, we present the second cycle of the design-based research (see also Keskitalo, Ruokamo, & Gaba, 2014). The case study was organised at Stanford University (Palo Alto, CA, USA) in 2009–2010 and involved nine facilitators and 25 students. During the case study, we collected and analysed data using quantitative and qualitative methods.
What follows is the introduction of the initial pedagogical model. Then we briefly summarise and explain the methods used during our second case study. Next, we introduce the redesigned pedagogical model, which is the result of these two design-based research cycles and various background studies (Keskitalo, 2011; Keskitalo, 2012; Keskitalo, Ruokamo, Väisänen, & Gaba, 2013). Finally, we draw conclusions and provide suggestions for future research.
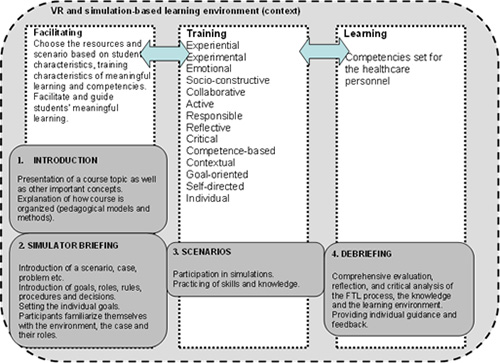
The purpose of this study was to understand teaching and learning in SBLEs in order to develop a pedagogical model. The initial pedagogical model is named the Facilitating, Training and Learning (FTL) model. The principles of the FTL model are derived from teaching, studying and learning (TSL) processes (Kansanen, Tirri, Meri, Krokfors, Husu, & Jyrhämä, 2000; Uljens, 1997) as well as the characteristics of meaningful learning (Ausubel, 1968; Jonassen, 1995; Löfström & Nevgi, 2007; Ruokamo & Pohjolainen, 2000) and previous pedagogical models (Joyce et al., 2002; Dieckmann, 2009). Generally, the model and research were based on socio-constructivist and socio-cultural perspectives on learning (Lave & Wenger, 1991; Vygotsky, 1978; Wells & Claxton, 2002). Figure 1 presents the FTL model for a virtual reality (VR) and simulation-based learning environment for healthcare after the first cycle of our design-based research (Keskitalo et al., 2010):
Figure 1. Facilitating, Training and Learning (FTL) model for VR and simulation-based learning (Keskitalo et al., 2010)
As the FTL process implies, students’ activity is necessary for learning to occur. In this context, we refer to teaching as facilitating (cf. Kansanen et al., 2000; Uljens, 1997), since teaching in a simulation-based learning environment is more an act of facilitating student learning. During the instructional process, facilitators are responsible for planning, guiding and evaluating the students’ learning process as well as reflecting on their own performance as facilitators (cf. Tissari et al., 2005). In the FTL model, studying is referred to as training (cf. Kansanen et al., 2000; Uljens, 1997), because in this context the students’ activity also involves training to master the specific skills needed in healthcare. In this model, training is described with 14 characteristics of meaningful learning (Hakkarainen, 2007; Jonassen, 1995; Löfström & Nevgi, 2007; Ruokamo & Pohjolainen, 2000; Tissari et al., 2005): experiential, experimental, emotional, socio-constructive, collaborative, active, responsible, reflective, critical, competence-based, contextual, goal-oriented, self-directed and individual(for a more detailed description, see Keskitalo et al., 2010; Keskitalo et al., 2014). We assert that facilitators should emphasise these characteristics in order to promote students’ meaningful learning in these learning environments. However, as previous studies have shown, these characteristics are partially intertwined and overlap (Jonassen, 1995).
Simulation-based courses are typically structured into four phases (introduction, simulator briefing, scenarios and debriefing), as suggested by Joyce et al.’s (2002) Learning through Simulation model (see also Dieckmann, 2009; Laurillard, 2012). Therefore, we embedded these phases in the FTL model in order to structure the learning event. During the first phase, the facilitator presents the course topic and the most important concepts and explains the simulation to the students. This phase should include explanations of how the course is organised as well as what type of pedagogical models and methods are used. During the simulator briefing, participants familiarise themselves with the simulation and have hands-on-time with the environment and the equipment. During this phase, the facilitator broadly introduces the scenarios. After the simulator briefing phase, students need to know and understand what is expected of them. In the scenarios phase, the students participate in the simulation, whereas the facilitator guides and monitors the students’ performance. In the final phase, the debriefing, the facilitator encourages the students to analyse the learning process and possibly set new learning goals (Fanning & Gaba, 2007). In the FTL model, the introduction and simulator briefings are led by the facilitator, whereas the training is student-centred. The debriefing phase is situated under the learning phase, since it is presupposed that learning will occur mostly during the debriefing as the students reflect on their own learning.
We set multiple research tasks in order to answer the following research question: What type of pedagogical model supports facilitation and students’ meaningful learning in SBLEs? The study used the design-based research (DBR) (Brown, 1992; Collins et al., 2004; Design-based Research Collective, 2003) and case study approaches (Gray, 2004; Yin, 2013). During this study, data were collected through case studies, and the development of the pedagogical model was an iterative process, as suggested by the DBR approach. In this study, we analyse the data collected during our second case study at Stanford University in 2009–2010. Since the original article (Keskitalo et al., 2014) focused more on the evaluation, from the perspectives of facilitators and students, the meaningfulness of simulation-based learning, this article focuses on the elaboration and evolution of the model across studies based on the results. In this article, we use some of the same data but also synthesise the knowledge gained from our previous studies (e.g. Keskitalo, 2011, 2012; Keskitalo et al., 2013).
Set-up and Participants
In the second case study, the students (n = 25) were mainly second-year anaesthesia residents and third- and fourth-year medical students. The students were studying anaesthesia crisis resource management and emergency medicine and participating in an anaesthesia internship; the facilitators’ (n = 9) specialties were anaesthesia, surgery and nursing. The youngest student respondent was 26 years old and the oldest 38 years old. Most of the students had no prior experience (20%) or had had exposure to no more than two simulation-based courses (64%). Altogether, the data were collected from five different courses, which lasted from three to nine hours. During the courses, all activities were done in a group format created by the facilitators. During the scenarios, usually one student had a leading role (the “hot seat” person) and called on others to help. The students who did not participate in the scenario watched it in a separate room via television. Before the study, research permission was applied for, and the study was approved by the institutional review board. Then, consent was obtained from the participants.
Simulation-based Learning Environments
Data were collected at two Stanford University simulation centres between February and March of 2010: the Patient Simulation Center of Innovation and the Goodman Surgical Simulation Center (see cisl.stanford.edu/about/centers.html). The Patient Simulation Center of Innovation is situated in the Veterans Affairs (VA) Palo Alto Health Care System. The centre has two large simulation rooms: one set up as an operating room and one as an intensive care unit, emergency department or ward. The centre also has five computer-directed patient simulators: three permanently set up and one adult simulator for in-situ training exercises in actual clinical environments. The centre also provides an infant simulator for paediatric anaesthesia training. The simulation centre has concentrated training in anaesthesiology, intensive care and rapid response teams, emergency medicine and respiratory therapy.
Data were also collected at the Goodman Surgical Simulation Center, which is situated in the middle of Stanford Hospital. The centre allows for convenient drop-in practice and pre-surgical planning. The skills area is open 24/7 (via card access) to all surgical residents. In addition to the centre’s accessibility, two surgical education fellows are available at the centre every day. The centre has vascular trainers, virtual reality laparoscopic trainers, box trainers, colonoscopy trainers and two patient simulators. It is used by surgical residents, medical students, residents in other disciplines, nursing professionals, respiratory therapists and others. Surgical residents, for example, have a weekly exercise time. During this period, they practice skills and decision making relevant to their surgical rotation in the simulation centre.
In this study, one room was used and equipped for students to rehearse. The room contained a patient simulator, and the vital signs were displayed on a monitor. Next to this room was an area in which the facilitator and the simulation operator controlled the simulator and guided the students’ learning process via audio devices. One room was dedicated to debriefing, where appropriate technology, such as video and audio-recording devices, was available. During this study, video and audio recordings were used during the debriefing sessions to complement the students’ reflection process.
Data Collection and Analysis
Empirical data were collected from facilitators and students using group interviews (one individual interview), observations, video recordings and pre- and post-questionnaires. For this study, we analysed 1) group interviews and one individual interview, 2) field notes and 3) post-questionnaires (see Table 1). The data analysis focused on the meaningfulness of the simulation-based courses as well as the evolution of the pedagogical model based on the lessons learned.
Table 1. Data collection and analysis methods as well as data sources (applied from Keskitalo et al., 2014)
|
Data Collection Method |
Data Source |
Data Analysis Method |
|
Group Interviews, one individual interview |
Facilitators (n = 9) Students (n = 16) 2 Anaesthesia Crisis Resource Management II courses, 2 Emergency Medicine courses, 1 Anaesthesia internship |
Atlas.ti qualitative coding and analysis software Qualitative content analysis |
|
Field notes |
Facilitators (n = 9) Students (n = 25) 2 Anaesthesia Crisis Resource Management II courses, 2 Emergency Medicine courses, 1 Anaesthesia internship |
Qualitative content analysis |
|
Post-questionnaires |
Students (n = 25) 2 Anaesthesia Crisis Resource Management II courses, 2 Emergency Medicine courses, 1 Anaesthesia internship |
Descriptive statistics |
The data analysis involved transcription of the collected data by an English-language transcription service. We analysed the interviews and field notes from the viewpoint of meaningful learning and the development of the pedagogical model, using the qualitative data analysis software Atlas.ti and a qualitative content analysis method. Content analysis is often understood as a systematic and objective analysis of the visible and obvious components of the text (e.g. Graneheim & Lundman, 2004; Gray, 2004). However, for some authors (Graneheim & Lundman, 2004) qualitative content analysis also interprets the underlying meaning of the text. The data analysis was an iterative process in which we organised and compressed the data into codes and categories and finally into themes. The unit of analysis was the utterance of the facilitator or student or the note made by the researcher reflecting the characteristics of meaningful learning or the pedagogical model. More profound data analysis process descriptions can be found in Keskitalo et al. (2014).
The questionnaires consisted of Likert-type questions related to expectations and experiences of the FTL process in an SBLE. Each of the 52 statements was scored on a continuum (1 = does not describe my expectations at all, 5 = describes my expectations very well). In addition, 29 Likert-type questions (0 = not at all, 5 = to a great extent) focused on the emotions students experienced during the course. The students were asked to evaluate the degree to which they felt a given emotion (e.g. enjoyment of studying, boredom, sense of community etc.) before and after the course. Five questions were also aimed at collecting students’ background information, and one open question gave the students space to write any other comments they had. For further analysis, we selected statements that reflected the characteristics of meaningful learning from the post-questionnaires (see also Hakkarainen, 2007; Nevgi & Löfström, 2005). The data were analysed using means, medians and standard deviations.
The results suggest that simulation-based learning is fundamentally meaningful since it inherently supports many characteristics of meaningful learning (see Table 2).
Table 2. Mean and median (standard deviation) ratings of meaningful learning characteristics after the course
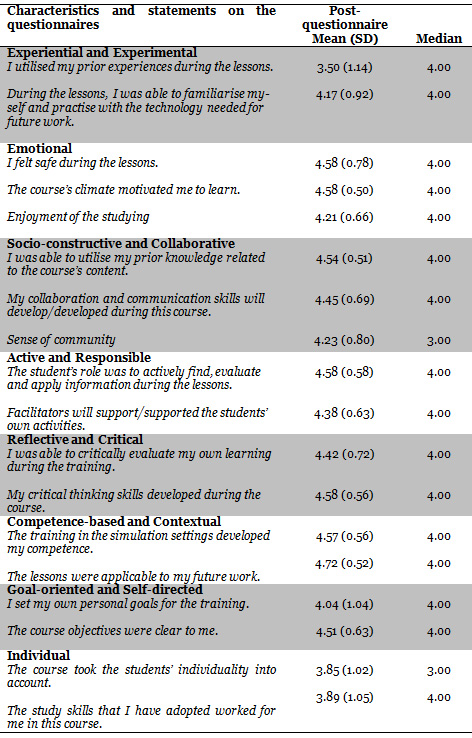
The analysis of the post-questionnaires suggested simulation-based learning was very meaningful (M = 3.50–4.72; SD = 0.52–1.14) for the students. The median values were also high (Md = 3–4). In two of the statements (Sense of community and The course took the students’ individuality into account) median values were 3.00, but in other statements they were 4.00. The lowest-rated variable was I utilised my prior experiences during the lessons (M = 3.50; SD = 1.14), which indicated that students utilised their prior experiences to some level. Since the standard deviation was high, the results suggest that some students felt that they utilised their previous experience during the course, while the others felt the opposite. However, this may also indicate that things were so new that the students needed to learn a lot and the relation to previous experiences was ambiguous. The highest-rated variable was The lessons were applicable to my future work (M = 4.72; SD = 0.52), which indicates that courses were valued as highly useful by future physicians.
However, we observed that some characteristics need more focus (Keskitalo et al., 2010; Keskitalo et al., 2014). Particularly the qualitative data revealed that the goal-oriented, self-directed and individual characteristics may limit the meaningful learning experience for some students. In the evaluated courses, formal articulation of the learning goals was poor, which in turn prevented students from setting their own learning goals, as a student observed:
But we didn’t know what today was going to be, so we couldn’t have specific objectives for today. (Group interview 2, students)
As noted, the poor articulation of the learning objectives and course description prevented some students from setting their own learning goals. This, in turn, had an adverse effect on the self-directed characteristics to be realised. To aid self-directed learning, facilitators should help students follow and evaluate their own learning in relation to the course’s objectives, their own goals and their own competency level (cf. Brockett & Hiemstra, 1991; Jonassen, 1995).
The analysis of the post-questionnaires also revealed that the individual characteristic was realised, but not more obviously than other characteristics (M = 3.85–3.89; SD 1.02–1.05; see Table 2). In this case, the median was also 3.00. Qualitative data support these results, since some students expected more individual guidance than was provided. The standard deviation was also high, which suggests that some students might have been satisfied, but others expected more support in the future, as the following excerpts clarify:
I think they just treated us all the same, basically. (Group interview 2, students)
Yeah. And I also think what’s interesting about this place is that the quality of resident they get here is not varied amongst—compared to other schools. And so, I don't think they have to worry as much about training toward—or putting simulators to individuals and individualising them to make them more improved based on their weaknesses and working on the simulator to improve the weaknesses of an individual, because I think that from the standpoint of the residency itself and the people in the residency, we’re all strong. (Group interview 1, students)
The instructional processes of the courses followed the Learning through Simulation model (cf. Joyce et al., 2001) quite obviously. It became clear that simulation-based learning includes at least the introduction, simulator and scenario briefing, scenarios and debriefing phases. Facilitators observed:
So that the morning time is going to be team building, gathering around the table having breakfast, signing forms, then to more of a traditional didactic or multimedia type of learning session. Then the rest of the day, simulations followed by debriefs. So, in the introduction period while they’re signing forms, there is a briefing as to what the expectations are. I didn't do it today, but I often will—prior to the first debriefing... So you’ve had a 25-35-minute scenario, we’re going to spend a similar amount of time talking about it. (Group interview 2, facilitators)
As the excerpts show and as we observed, short lectures can occur between the familiarisation and actual scenarios. In this particular course (anaesthesia crisis resource management), the lectures dealt with principles of crisis recourse management and communication issues within healthcare.
The other theoretical viewpoints that facilitators mentioned were adult learning and experiential learning principles (cf. Kolb, 1984). Kolb’s experiential learning cycles are viewed as a useful framework within simulation-based learning in healthcare. In simulation-based education, simulations are viewed as concrete experiences that are debriefed afterward (e.g. Zigmont, Kappus, & Sudikoff, 2011). This also enhanced the experiential and reflective characteristics of meaningful learning to be realised in terms of gaining new experiences within the simulation and discussing them afterward. In terms of adult education, mature learners benefit from the student-centred approach (because of age, maturity, life experiences, multiple responsibilities etc.; see Knowles, Holton, & Swanson, 1998), thus placing pressure on individualised guidance as well.
The aim of the pedagogical model was to shed light on the important learning theories that are essential when organising teaching and learning in simulation-based learning environments. The aim was to also conceptualise meaningful simulation-based learning and define characteristics that can be useful in simulation-based learning environments in healthcare. In terms of the lesson learner, we took the deficiencies of the previous model into account and redesigned our initial FTL model. The redesigned model is presented in Figure 2.
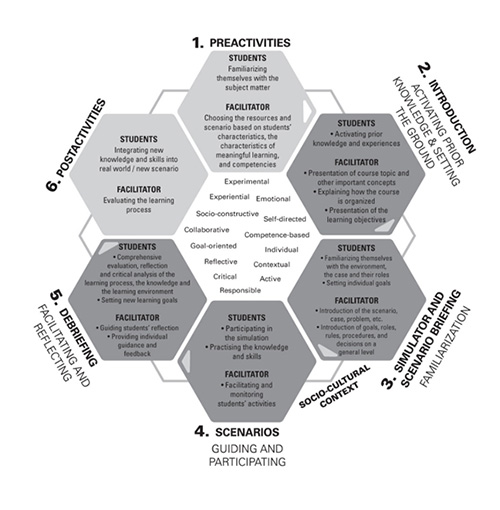
Figure 2. The pedagogical model for simulation-based learning in healthcare (Keskitalo, 2015)
First, the FTL model was not tested thoroughly; therefore, we decided that naming the pedagogical model in this phase was not appropriate. After several design-based research cycles, it will be more appropriate to name the model.
The research and the first design were based on socio-constructivist and socio-cultural theories of learning (Lave & Wenger, 1991; Palincsar, 1998; Vygotsky, 1978; Wells & Claxton, 2002). These theories place learning in a wider socio-cultural context and view knowledge as the result of a shared and contextually bound process of knowledge construction rather than solely an individual experience. However, this did not become clear enough in our previous model (see Figure 1). Therefore, in the redesigned model (see Figure 2) we emphasised that learning is a contextually bound and tool-dependent process by surrounding the pedagogical model with a socio-cultural context. The socio-cultural perspective helps us understand the complexity of learning and the development of expertise and how the tools, practices and institutions also constantly changed within this interplay (Palincsar, 1998).
The characteristics of meaningful learning were chosen as a general framework within the pedagogical model, because they can help bring to the forefront issues known to enhance learning (e.g. Jonassen, 1995). Based on this study and our previous studies (Keskitalo et al., 2010; Keskitalo et al., 2014), SBLEs seem to be ideal environments for meaningful learning. However, the goal-oriented, self-directed and individual characteristics need more attention. Therefore, in order to realise the goal-oriented characteristic, in future simulation-based courses the goals should be stated clearly, and they should be reflected on during the debriefing process. Furthermore, participants could benefit from setting their own learning goals in relation to the course’s objective and their own level of expertise. However, this was what we found during our first case study, and based on the results, the FTL model was refined (Keskitalo et al., 2010). Learning is also very much an individual process (De Corte, 1995), and some students might expect more individualised feedback about their performance as well as guidance on how to develop their skills and knowledge further (cf. Keskitalo et al., 2010; Keskitalo et al., 2011). In other words, we have clarified in the redesigned pedagogical model things that facilitators can do to help realise the goal-oriented, self-directed and individual characteristics of meaningful learning.
At this point, we also realised that the characteristics of meaningful learning not only describe and are restricted to the planning and implementation of students’ training (the phase when they are most active) but also can be taken into account from the beginning of the course to the end. Therefore, we placed the characteristics at the centre of the pedagogical model (see Figure 2). As a consequence, we also discarded the FTL process from our redesigned model (cf. FTL model, Figure 1), since it did not provide any additional value to the model. The original teaching, studying and learning process is more related to classroom-based teaching (Kansanen et al., 2000), with the aim of the division to accentuate students’ own activity. However, simulation-based learning environments in healthcare are based on students’ activity and, therefore, are a natural part.
In contrast to the FTL model’s four phases (see Figure 1), the redesigned pedagogical model (see Figure 2) consists of six distinct phases: pre-activities, introduction, simulator and scenario briefing, scenarios, debriefing and post-activities. For the redesigned model, we added facilitators’ and students’ pre-activities and post-activities. These phases are highly relevant for students’ learning and development in simulation-based education; therefore, we wanted to shed light on those activities as well. During the pre-activities phase, the facilitators are responsible for planning the learning process—for example, choosing the resources and learning material and organising the environment. However, students are responsible for having adequate knowledge and skills when they participate in simulation-based education. Facilitators should critically evaluate the entire instructional process as post-activities (cf. Keskitalo et al., 2010) in order to develop their teaching style (Boese et al., 2013); whereas students prefer to test their learned knowledge and skills in a new scenario or in real life as post-activities (see Kolb, 1984; Merrill, 2002).
The study’s results should be read with caution, since this case study had both strengths and weaknesses. A clear strength of the study was that it produced various types of data and provided many angles from which to look at the phenomenon. However, large amounts of data can be overwhelming, especially in design-based research (Barab & Squire, 2004; Collins et al., 2004). Therefore, in this study we focused on interviews, field notes and post-questionnaires. However, this study also had weaknesses. One major weakness was that despite our expectations, we could not organise an appropriate teaching experiment and test the model adequately. Therefore, we discuss the use of the design-based research approach instead of applying a pure method. Thus, the data collection is best described as a case study, and to develop the pedagogical model, we used the iterative nature of the design-based research method. In addition, the quantitative analysis of post-questionnaires is simply descriptive; therefore, the results of this study should be interpreted and adapted carefully.
The main result of this study was the redesigned pedagogical model. With the help of this model, healthcare education practitioners can make informed choices about simulation-based education. The model can also be used to identify gaps that must be reconsidered and developed in simulation-based education. In other words, the pedagogical model ensures that a more holistic and meaningful approach to teaching and learning is adopted. However, the model requires evidence and further development.
Ausubel, D. P. (1968). Educational psychology: A cognitive view. New York: Holt, Rinehart & Winston.
Brenner, M., Brown, J., & Canter, D. (1985). The research interview. London: Academic Press.
Brewer, E. P. (2011). Successful techniques for using human patient simulation in nursing education. Journal of Nursing Scholarship, 43(3), 311–317.
Brockett, R. G., & Hiemstra, R. (1991). Self-direction in adult learning: Perspectives on theory, research, and practice. London: Routledge.
Brown, A. L. (1992). Design experiments: Theoretical and methodological challenges in creating complex interventions in classroom settings. Journal of the Learning Sciences, 2(2), 141–178.
Cohen, L., Manion, L., & Morrison, K. (2011). Research methods in education. (7th ed.). London/New York: RoutledgeFalmer.
Collins, A., Joseph, D., & Bielaczyc K. (2004). Design research: Theoretical and methodo-logical issues. The Journal of the Learning Sciences, 13(1), 15–42.
Cook, D. A., Hatala, R., Brydges, R., Zendejas, B., Szostek, J. H., Wang, A. T., Erwin, P. J., & Hamstra, S. J. (2011). Technology-enhanced simulation for health professions education: A systematic review and meta-analysis. The Journal of the American Medical Association (JAMA), 306(9), 979–988.
De Corte, E. (1995). Fostering cognitive growth: A perspective from research on mathematics learning and instruction. Educational Psychologist, 30(1), 37–46.
Design-based Research Collective. (2003). Design-based Research: An emerging paradigm for educational inquiry. Educational Research, 32, 5–8.
Dieckmann, P. (2009). Simulation setting for learning in acute medical care. In P. Dieckmann (Ed.), Using Simulations for Education, Training and Research (pp. 40–138). Lengerich, Germany: Pabst Science Publishers.
Eaves, R. H., & Flagg, A. J. (2001). The U.S. Air Force pilot simulated medical unit: A teaching strategy with multiple applications. Journal of Nursing Education, 40(3), 110–116.
Fanning, R. M., & Gaba, D. M. (2007). The role of debriefing in simulation-based learning. Simulation in Healthcare, 2(2), 115–125.
Flick, U. (1998). Introduction to qualitative research. London: Sage.
Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2), 105–112.
Gray, D. E. (2004). Doing research in the real world. London: Sage Publications.
Hakkarainen, P. (2007). Promoting meaningful learning through the integrated use of digital videos. Doctoral dissertation, University of Lapland. Acta Universitatis Lappoensis 121. University of Lapland, Faculty of Education, Finland. Rovaniemi: University of Lapland Printing Centre.
Hayden, J. K., Smiley, R. A., Alexander, M., Kardong-Edgren, S., & Jeffries, P. R. (2014). The NCSBN National Simulation Study: A longitudinal, randomized, controlled study replacing clinical hours with simulation in prelicensure nursing education. Journal of Nursing Regulation, 5(2), 1–66.
Jonassen, D. H. (1995). Supporting communities of learners with technology: A vision for integrating technology with learning in schools. Educational Technology, 35(4), 60–63.
Joyce, B., Calhoun, E., & Hopkins, D. (2002). Models of learning—tools for teaching. (2nd ed.). Buckingham: Open University Press.
Kansanen, P., Tirri, K., Meri, M., Krokfors, L., Husu, J., & Jyrhämä, R. (2000). Teachers’ pedagogical thinking. Theoretical landscapes, practical challenges. American University Studies. Series XIV, Educational vol. 47. New York: Peter Lang.
Ker, J. (2012). Review: The challenges of developing and evaluating complex care scenarios using simulation in nurse education. Journal of Research in Nursing, 17(4), 346–347.
Keskitalo, T. (2011). Teachers’ conceptions and their approaches to teaching in virtual reality and simulation-based learning environments. Teachers and Teaching: Theory and Practice, 17(1), 131–147.
Keskitalo, T. (2012). Students’ expectations of the learning process in virtual reality and simulation-based learning environments. Australasian Journal of Educational Technology, 28(5), 841–856.
Keskitalo, T. (2015). Designing a pedagogical model simulation-based healthcare education. Acta Universitatis Lapponiensis 299. Rovaniemi: Lapland University Press.
Keskitalo, T., Ruokamo, H., & Gaba, D. (2014). Towards meaningful simulation-based learning with medical students and junior physicians. Medical Teacher, 36(3), 230–239.
Keskitalo, T., Ruokamo, H., & Väisänen, O. (2010). How does the facilitating, training and learning model support characteristics of meaningful learning in a simulation-based learning environment from facilitators’ and students’ perspectives? Proceedings of ED-Media 2010: World Conference on Educational Multimedia, Hypermedia & Telecommunications. June 27–July 1, 2010, Toronto, Canada (pp. 1736–1746). Chesapeake, VA: AACE.
Keskitalo, T., Ruokamo, H., Väisänen, O., & Gaba, D. (2013). Healthcare facilitators’ and students’ conceptions of teaching and learning—An international case study. International Journal of Educational Research, 62, 175–186.
Kolb, D. A. (1984).Experiential learning: Experiences as a source of learning and development. Englewood Cliffs. N. J.: Prentice Hall.
Konia, M., & Yao, A. (2013). Simulation a new educational paradigm? The Journal of Bio-medical Research, 27(2), 75–80.
Knowles, M. S., Holton, E. F., & Swanson, R. A. (1998). The adult learner (5th ed.).Houston, TX: Gulf.
Laurillard, D. (2012). Teaching as a design science: Building pedagogical patterns for learning and technology. New York: Routledge.
Lave, J., & Wenger, E. (1991). Situated learning: Legitimate peripheral participation. Cambridge: Cambridge University Press.
Lincoln, Y., & Guba E. (1985). Naturalistics inquiry. Newberry Park, CA: Sage.
Löfström, E., & Nevgi, A. (2007). From strategic planning to meaningful learning: Diverse perspectives on the development of web-based teaching and learning in higher education. British Journal of Educational Technology, 38(2), 312–324.
Nevgi, A., & Löfström, E. (2005). The quality of online learning: Teachers’ and students’ evaluation of meaningful learning experiences in web-based course. In S. Kiefer, J. Michalak, A. Sabanci, & K. Winter (Eds.), Analysis of educational policies in comparative educational perspective (pp. 187–203). Linz: Trauner.
Paige, J. T., Arora, S., Fernandez, G., & Seymour, N. (2015). Debriefing 101: Training faculty to promote learning in simulation-based training. American Journal of Surgery, 209(1), 126–131.
Palincsar, A. S. (1998). Social constructivist perspectives on teaching and learning. Annual Review of Psychology, 49(1), 345–375.
Ruokamo, H., & Pohjolainen, S. (2000). Distance learning in multimedia networks project: Main results. British Journal of Educational Technology, 31(1), 17–125.
Tissari, V., Vahtivuori-Hänninen, S., Vaattovaara, V., Ruokamo, H., & Tella, S. (2005). Applying pedagogical models in network-based education: Research findings from the Finnish HelLa project case studies. In P. Kommers & G. Richards (Eds.), Proceedings of ED-MEDIA 2005: World Conference on Educational Multimedia, Hypermedia & Telecommunications 2005 (pp. 656–663). Chesapeake, VA: AACE.
Uljens, M. (1997). School didactics and learning. Hove, East Sussex: Psychology Press.
Vygotski, L. (1978). Mind in society: The development of higher psychological processes. Cambridge: Harvard University Press.
Wells, G., & Claxton, G. (2002). Learning for life in 21st century. Sociocultural perspectives on the future of education. Cambridge, MA: Blackwell.
Yin, R. K. (2013). Case study research: Design and methods (5th edition). Thousand Oaks, California: Sage.
Zigmont, J. J., Kappus, L. J., & Sudikoff, S. N. (2011). Theoretical foundations of learning through simulation. Seminars in Perinatology, 35(2), 47–51.